-
Scleral Lens Workshop in Germany
I was invited to lecture at a scleral lens workshop in Munich Germany this past November
-
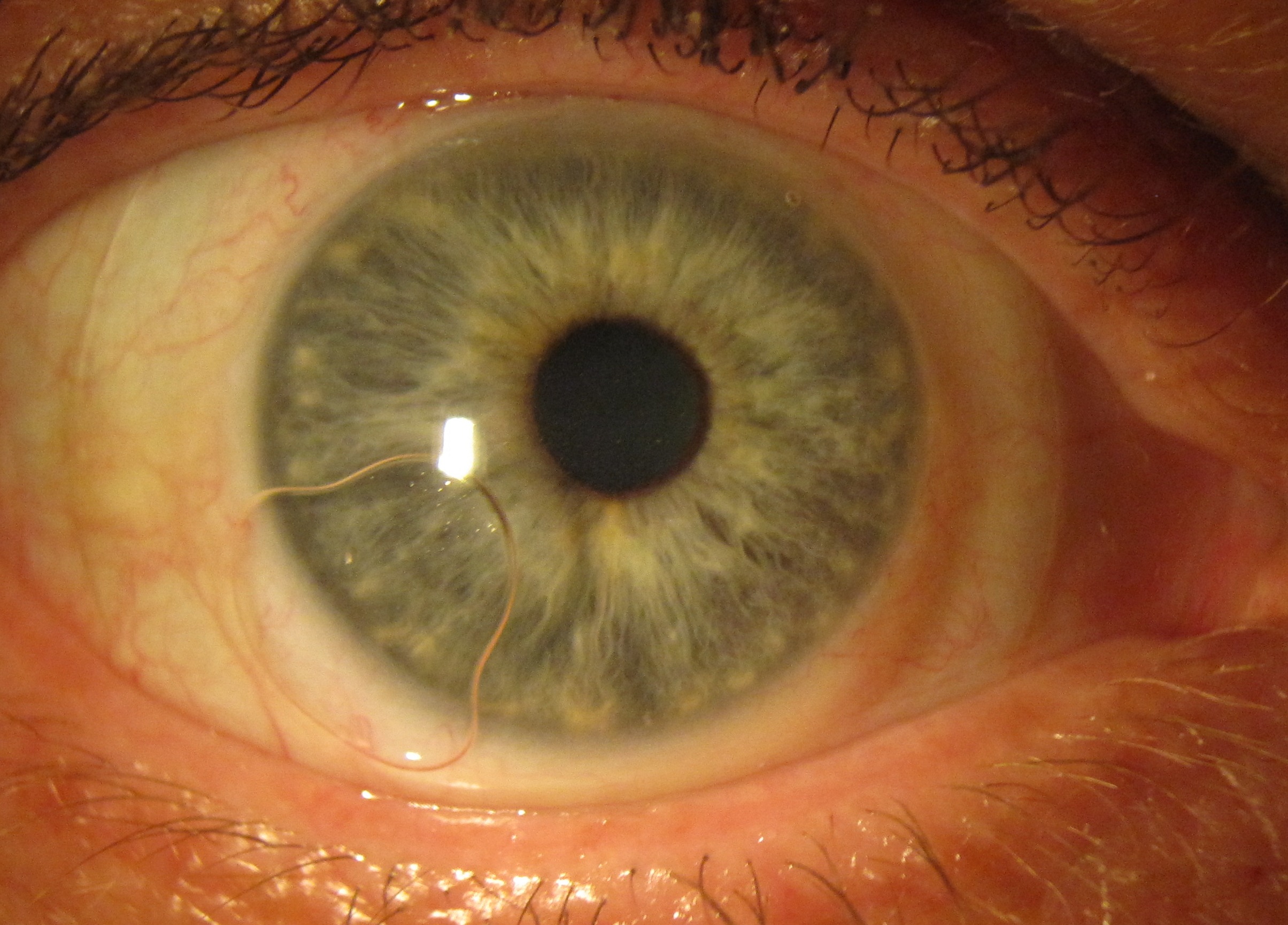
Wavefront corrected scleral lenses
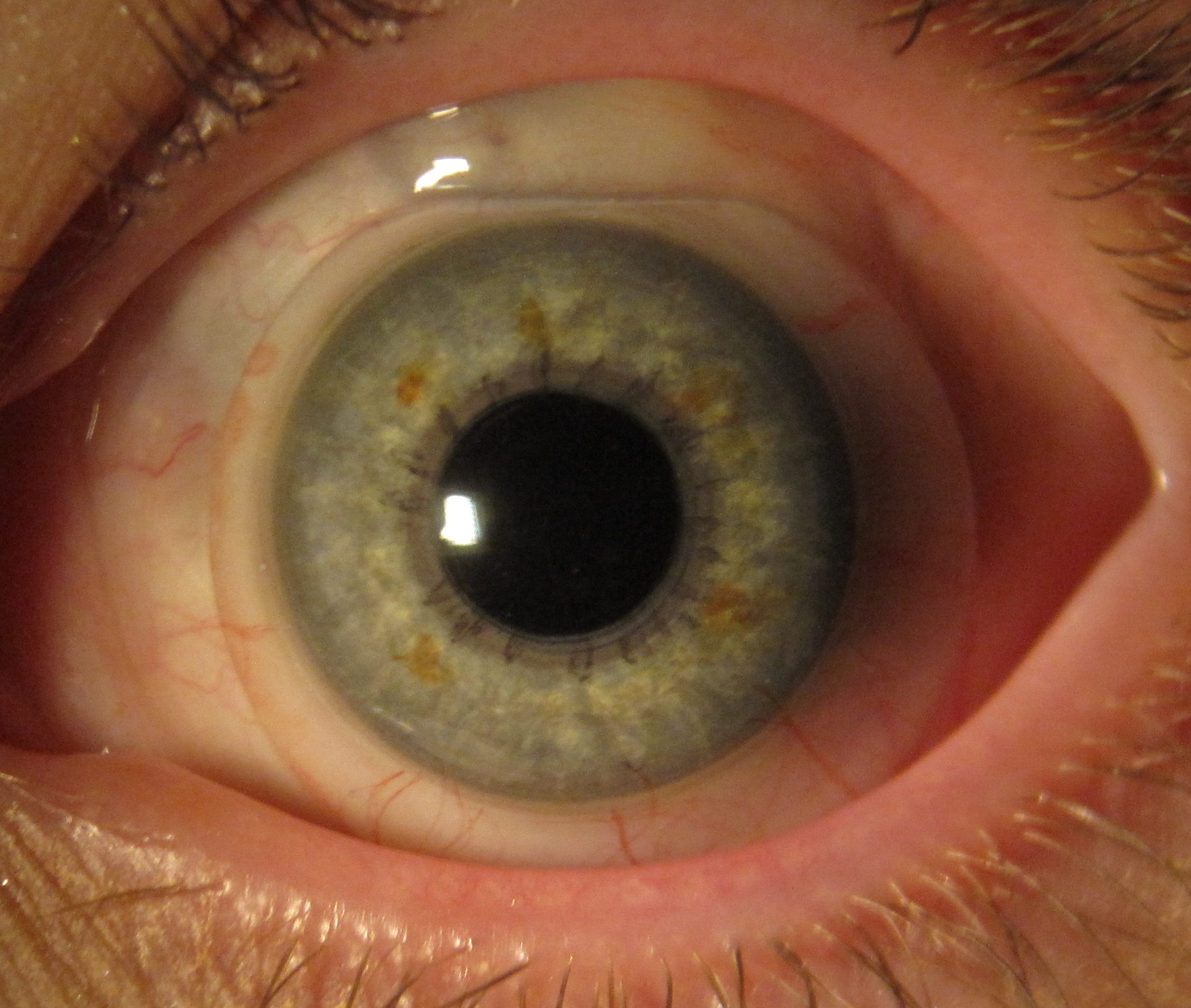
Wavefront corrected scleral lenses I’m now able to offer patients highly customized optics in the form of wavefront correction to improve visual acuity for eyes that have residual higher order aberrations with scleral lenses.
-
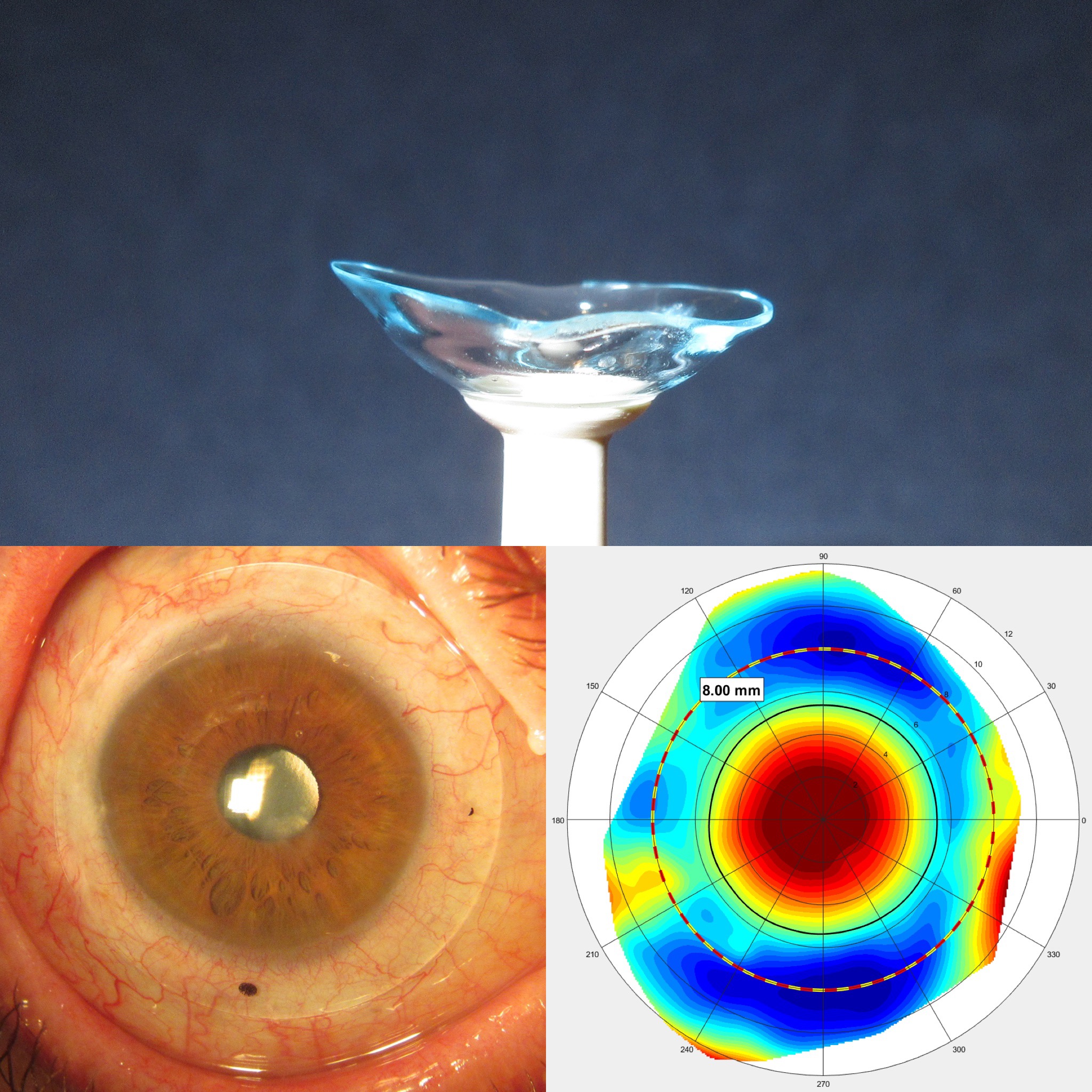
Latitude
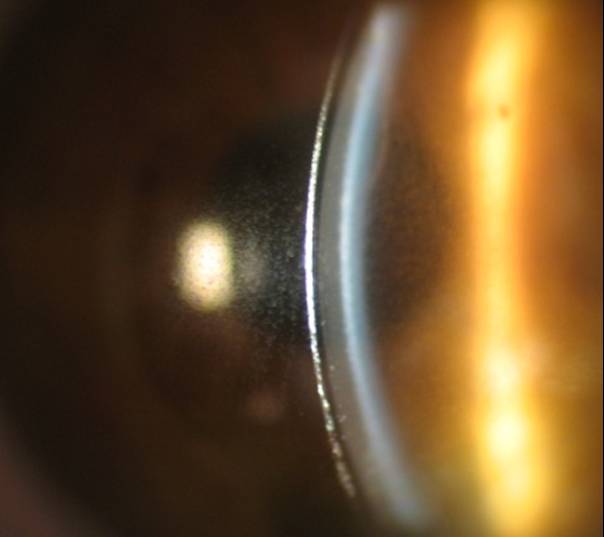
I am now fitting the Latitude scleral lens, which is a free-form completely customized scleral contact lens designed from sMap3D corneo-scleral topography measurements. The Latitude lens is uniquely designed to fit each individual eye providing improved comfort and satisfaction, even for the most extreme fits.
-
Argentina
During November I had the opportunity to speak to eye care practitioners in Buenos Aires Argentina about fitting scleral contact lenses.
-
France
During September I had the chance to speak with some of the best scleral lens fitters in the world for the European Contact Lens Society of Ophthalmologist held in Mandelieu la Napoule France.
-
Rome
I had the opportunity to lecture at the Italian Scleral Lens society. Many of the foremost scleral lens experts in the world attended. Rome Italy
-
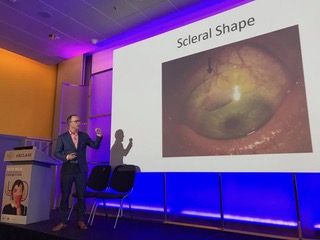
SSSG- Qualtitative Shape
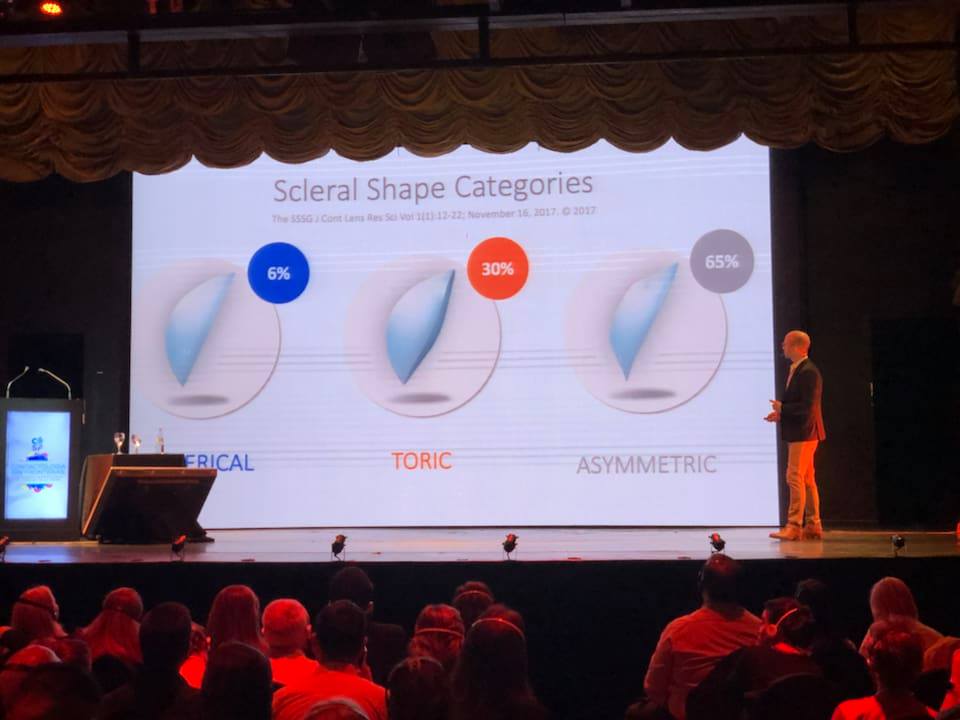
The Scleral Shape Study Group- An international panel of experts on scleral shape, which includes: Greg DeNaeyer, Don Sanders, Eef van der Worp, Jason Jedlicka, Langis Michaud, and Sheila Morrison- recently published a paper on the analysis of scleral shape. The findings of the study suggest that a majority of patients may benefit from scleral lenses that are beyond spherical or toric back surface designs.
-
BCLA/ISCLS meetings
I had the chance to lecture on new research that we are investigating regarding scleral shape in Scotland and England this last month. It was insightful to discuss scleral lenses with my international colleagues.
-
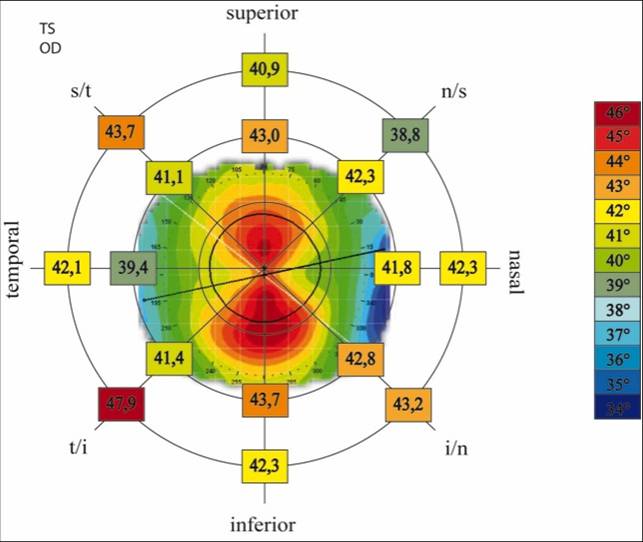
sMap3D Corneo-Scleral Topographer
I am now using the sMap3D corneo-scleral topographer to measure, analyze, and fit custom scleral lenses. Using this technology is a giant leap forward for fitting scleral contact lenses. Ultimately this tailored approach to fitting scleral lenses improves fit, comfort, and overall patient satisfaction. Check out this case report from my friends Pat and Mark- A New Look at Scleral Shape
-
NCC- Netherlands
I just back from lecturing on scleral lenses at the NCC meeting held in Veldhoven Netherlands. The two day contact lens conference attracted approximately 1500 practitioners.